
Ask most dental clinic owners what their biggest operational problems are and you will hear the usual answers. No-shows. Low treatment acceptance. Staff inefficiency. Front desk overload.
Rarely does anyone mention the prescription pad.
Yet in most clinics, the prescription pad sits at the exact intersection of clinical risk, legal exposure, and operational fragmentation. A dentist scribbles out a prescription after a procedure. The patient leaves with a piece of paper. No record is created in the patient file. No one checks for drug interactions. No one knows, six months later, what was prescribed, at what dosage, or whether the patient ever filled it.
This is not a small administrative problem. It is a compliance gap. And in an era where dental regulatory bodies are tightening documentation requirements, the paper prescription is increasingly a liability.
The shift in how dental AI practices are expected to manage prescriptions is not being driven by technology enthusiasm. It is being driven by three structural pressures.
First, regulatory frameworks in India, Singapore, the UAE, and several other markets are moving toward mandatory electronic prescribing for controlled substances and increasingly signaling intent to extend that requirement across all clinical prescriptions. Practices that have not built the infrastructure now will be retrofitting it under pressure later.
Second, dental chains and multi-branch operators have created a new competitive baseline. A solo practitioner competing against a structured clinic network is being implicitly compared on care continuity, documentation quality, and follow-up reliability. Patients notice these differences, even if they cannot name them.
Third, patient records are increasingly being used in insurance claims, medico-legal disputes, and referral workflows. A prescription that exists only on paper is a record that, functionally, does not exist. The downstream cost of that gap shows up not at the time of writing the prescription, but months or years later.
In a paper-based workflow, the prescription is written after the consultation. It bears no connection to the diagnosis in the patient's file, the treatment plan discussed, or the clinical findings from that visit. If a dentist prescribes an antibiotic following an extraction, that prescription exists in isolation. It is not linked to the procedure, the patient's medical history, or any prior prescriptions.
This disconnection matters when a patient returns. The next appointment might be handled by a different dentist, or the original dentist seeing the patient six months later with no memory of the case. The prescription record is either missing or exists as a handwritten note in a physical file that no one will search before writing a new one.
Dentists routinely prescribe from a relatively short list of drugs: analgesics, antibiotics, anti-inflammatories, antifungals. The assumption is that this narrow formulary reduces interaction risk. That assumption is not always safe.
A patient on warfarin receiving a course of metronidazole faces a meaningful drug interaction risk. A patient on SSRIs receiving tramadol faces serotonin syndrome risk. These interactions are well-documented. They are also easily missed when a prescription is written by hand, from memory, without any cross-check against the patient's medication history.
Paper prescriptions provide no mechanism for flagging these interactions. The dentist is working entirely from recall, which is inconsistent by nature.
In a clinic with two or three dentists, each practitioner tends to develop their own prescribing patterns. One dentist prescribes amoxicillin at 500 mg TDS for five days. Another prescribes 250 mg TDS for seven days for a comparable indication. Neither is necessarily wrong. But the inconsistency is invisible because there is no system that makes it visible.
When a complaint arises or an audit is conducted, this inconsistency becomes a problem. It suggests a lack of clinical governance. It raises questions about whose protocol is correct and whether there is a protocol at all.
A patient leaves the clinic holding a handwritten prescription they may or may not be able to read. If they have questions about the medication, dosage, or duration, there is no reference document they can access later. If they lose the prescription, they either return to the clinic or skip the medication.
This is a retention problem as much as a clinical one. Every unresolved patient query that requires a callback or a return visit is an administrative cost. Every patient who abandons a post-procedure medication course is a potential complication that returns to the chair.
If a regulatory body, insurance provider, or plaintiff's attorney requests the prescribing history for a specific patient, what does a paper-based practice produce? Physical files, if they have not been misplaced, damaged, or misfiled. Incomplete records. No timestamp for when the prescription was written or by whom.
Electronic prescription records are not just cleaner. They are legally defensible in a way that paper records are not.
Electronic dental prescription management software does not just digitize the prescription pad. It changes the architecture of how prescribing decisions are made and recorded.
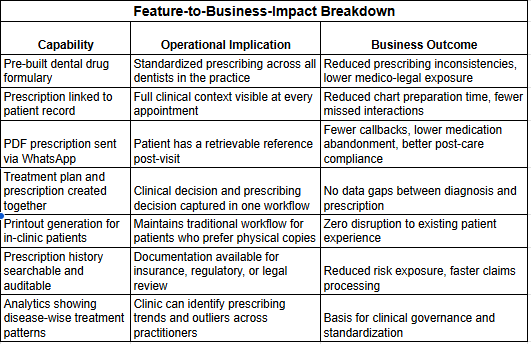
At the functional level, a modern e-prescription tool for dental practices maintains a pre-built drug formulary. The dentist selects from a curated set of medications relevant to dental treatment rather than writing from memory. This reduces transcription errors, standardizes dosage defaults, and creates consistency across all prescribers in the practice.
Prescription records are linked to the patient file at the point of creation. When a dentist opens a patient's profile before a consultation, the full prescribing history is visible alongside clinical notes, scan results, and treatment records. This is the foundation of care continuity. It is also the foundation of defensible documentation.
Practices using integrated platforms like scanO Engage, which centralizes patient records, prescriptions, treatment plans, and clinical data in a single workspace, see a measurable reduction in the time staff spend reconstructing patient history before appointments. The dentist walks into a consultation with full context, not a blank recall.
The prescription itself becomes a distributable document. Within the scanO Engage workflow, a completed prescription and treatment plan can be sent to the patient's WhatsApp as a PDF. The patient has a permanent reference they can show to a pharmacist, access during travel, or share with a specialist. The clinic retains a timestamped record of what was sent, when, and to whom.
A common mistake is treating electronic prescribing as an isolated module. It is not. The value of an e-prescription tool compounds when it is part of a connected clinical ecosystem.
Consider the workflow before a prescription is even written. A patient comes in for a scheduled appointment. If the practice uses AI-enabled appointment scheduling, the dentist already knows what the previous visit covered, what treatment was planned, and what was discussed. Automated reminders have reduced the likelihood of a no-show. Real-time confirmation tracking has given the front desk advance visibility into the day's case load.
By the time the dentist is with the patient, the consultation is informed by data, not just memory.
Platforms that integrate AI screening with practice management, as scanO Engage does through its connection with scanO air clinical data, allow a dentist to correlate a current scan finding with past scan findings, previous treatment notes, and prescribing history in a single view. When it is time to prescribe, the prescription is written with full context. Drug interactions can be cross-checked against the patient's recorded medical history. The completed prescription is sent to the patient via WhatsApp and stored against the appointment record.
The downstream effect of this integration is not just efficiency. It is risk reduction. Every prescription is traceable. Every clinical decision has an associated record. The practice has documentation that holds up to scrutiny.
For single-chair practices, the business case for electronic prescription management is largely about risk control and professionalism. For multi-branch operators, it is also about scalability.
A dental group running three or more locations cannot maintain clinical governance through informal protocols and personal relationships. When a dentist moves between branches, or when a patient visits a branch other than their usual one, care continuity depends on whether the records are centralized and accessible.
Paper-based systems break at this point. Each branch maintains its own files. Each dentist follows their own conventions. The group has no aggregate view of prescribing patterns, no ability to standardize dosage protocols across locations, and no clean audit trail.
Platforms designed for multi-branch management, where scanO Engage's dashboard architecture covers multi-branch and multi-chair operations, allow a group owner to see appointment volumes, disease-wise scan findings, and treatment activity across all locations. Prescription data feeds into this picture. A practice owner can identify which locations have the highest post-procedure complication callbacks, a proxy metric for prescribing quality and patient compliance, and address the outliers with protocol adjustments.
This is clinical governance at scale. It is only possible when prescription data is structured, centralized, and connected to the broader patient record.
There is a revenue argument for electronic prescription management that most clinic owners have not fully worked through.
Post-procedure prescriptions are a point of patient contact. When a patient receives a well-documented prescription, sees it on their phone, understands their medication schedule, and experiences no complications, their trust in the practice increases. Trust is the primary driver of recall compliance. Patients who trust their dentist return for check-ups. Patients who have a fragmented experience, unclear instructions, a lost prescription, an unexplained complication, often do not.
The connection between prescription quality and recall rates is indirect. It is also real.
Practices that close the loop at the prescription stage, confirming the patient has the document, making them aware of the follow-up timeline, connecting them to the patient app for ongoing communication, are building a recall infrastructure that paper-based prescribing cannot support.
When prescription records are linked to patient profiles that also track appointment history, call and chat communication, and scan results, as they are in an integrated platform, the practice has the data to run structured recall campaigns. Disease-wise analytics dashboards identify patients whose conditions have a known progression risk. These patients can be prioritized for proactive outreach.
The prescription is not the end of the clinical interaction. In a well-run practice, it is the beginning of the next one.
Dental practices that delay investment in electronic prescription management are not saving money. They are accumulating undisclosed risk.
The liability from a poorly documented prescription event, a drug interaction that was not flagged, a dosage inconsistency that gets surfaced in a complaint, a regulatory audit that produces incomplete records, rarely materializes as a routine operational cost. It materializes as a significant, concentrated one.
The investment in structured e-prescription infrastructure is not a large one relative to that risk. The shift from paper to a connected electronic system, particularly one that is already part of a broader practice management platform, is a configuration change as much as it is a procurement decision.
The practices that will face the least disruption from tightening regulatory requirements are the ones that are already operating on structured, auditable, clinically integrated systems.
3. How does scheduling software integrate with Dental AI systems?
Modern platforms connect with tools like Tissue Ai and screening devices to trigger structured follow ups and recall cycles.
Is switching to electronic prescriptions legally required for dental practices right now?
Requirements vary by country and region. Several markets have introduced mandatory e-prescribing for specific drug categories, and regulatory direction in most markets is moving toward broader electronic documentation requirements. More immediately, most dental regulatory bodies require complete and legible patient records, which paper prescriptions often fail to satisfy in practice. Moving to electronic prescriptions before a requirement exists is a lower-cost decision than scrambling to comply after one is introduced.
What happens if the software is unavailable or the internet goes down when I need to write a prescription?
A legitimate concern for any clinician. Most practice management platforms with e-prescription functionality maintain an offline mode or local data caching for exactly this scenario. Pre-loaded drug formularies mean the prescribing workflow can continue without a live connection. The prescription syncs to the patient record when connectivity is restored. Before adopting any platform, it is worth confirming how it handles offline scenarios specifically.
My clinic uses a relatively standard drug list. Is an e-prescription tool really necessary for a small practice?
The risk exposure from paper prescriptions does not scale with practice size. A single undocumented prescription that leads to a drug interaction or a complaint creates the same legal and professional consequences regardless of whether the clinic has one chair or ten. Small practices are, if anything, more vulnerable because they typically have less administrative infrastructure to absorb and document a complaint properly. The formulary pre-loading feature is particularly useful for solo practitioners because it removes the cognitive load of recalling dosage defaults under time pressure.
How does electronic prescribing connect to patient retention in practice?
When a patient leaves a consultation with a PDF of their prescription on WhatsApp, alongside their treatment plan and scan results, they have a tangible reference to the care they received. This reduces the volume of post-appointment queries to the front desk, reduces medication abandonment, and gives the patient something concrete to show a pharmacist or specialist. More importantly, it signals to the patient that the clinic's systems are organized. Patients who perceive a clinic as administratively reliable are measurably more likely to return for follow-up and recall appointments than patients who had to chase a paper document or re-explain their history at each visit.
An AI-powered co-author focused on generating data-backed insights and linguistic clarity.
Dr. Vidhi Bhanushali is the Co-Founder and Chief Dental Surgeon at scanO . A recipient of the Pierre Fauchard International Merit Award, she is a holistic dentist who believes that everyone should have access to oral healthcare, irrespective of class and geography. She strongly believes that tele-dentistry is the way to achieve that.Dr. Vidhi has also spoken at various dental colleges, addressing the dental fraternity about dental services and innovations. She is a keen researcher and has published various papers on recent advances in dentistry.








