
Most dental practices do not have a data problem. They have a visibility problem.
Production can look “fine” while the schedule quietly leaks chair time. Collections can look “stable” while aging receivables drift into the 60 to 90 day bucket. Case presentations can feel thorough while acceptance rates stall at average levels. The point of a dashboard is not to report activity. It is to reveal operational truth early enough to act.
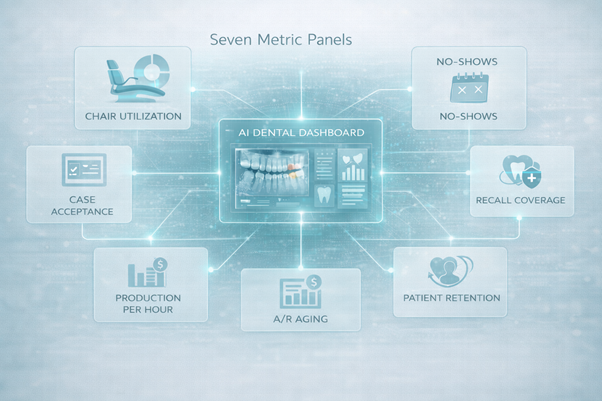
This is where dental AI has started to change expectations, not by adding more reports, but by making early operational risk visible at the daily level.
A packed calendar can still hide unproductive chair time. The operational issue is not whether you are booked. It is whether booked time converts into completed, billable care with minimal gaps.
Track chair utilization daily: scheduled hours vs productive hours, and “open chair time” by provider and by operatory. Even a10% utilization gap is expensive because overhead does not drop when the chair is empty. Dental overhead often sits around 60% to 65% of production, so unused capacity typically becomes pure margin loss. The consequence is predictable. Teams work harder, not better. Hygienists feel overbooked. Doctors feel rushed. Output still underperforms.
No-shows are not random. They cluster by time of day, lead time, procedure type, and patient segment. That makes them measurable and partially controllable.
Track cancellation and no-show rate daily, plus same-day fill rate. The American Dental Association has pointed to 5% or less as a benchmark for cancellation and no-shows. If your rate is above that, you are not just losing visits. You are forcing reactive scheduling, disrupting clinical flow, and inflating effective overhead because fixed costs spread across fewer completed appointments.
The consequence is more than revenue loss. It is lower clinical consistency and a team that spends its day recovering the schedule instead of running it.
Case acceptance is often treated as a communication skill problem. It is usually a systems problem: inconsistent presentation, unclear sequencing, weak financial pathways, and poor follow-up discipline.
Track case acceptance rate daily by category : restorative, elective, hygiene-driven treatment, and larger plans.
Bench marks commonly cited for general dentistry put average acceptance around 50% to60%, with high-performing practices in the 70% to 80% range.
The consequence of weak acceptance is not only lower production. It is a slower clinical pipeline, more rework in consultations, and a growing gap between diagnosed need and delivered care.
Recall is not an admin task. It is a demand engine. When recall breaks, restorative opportunity breaks with it.
Track active recall coverage daily: the percentage of hygiene patients who are already scheduled into the future, plus overdue recall count. The ADA highlights a practical target question: are 90%of recare patients scheduled at all times. When this number dips, the schedule maystill look full today, but future chair time becomes fragile.
The consequence is delayed diagnosis, fewer timely interceptive treatments, and a practice that becomes dependent on new patients to patch predictable recall leakage.
Daily production is a result. It does not explain why it happened, or whether it happened efficiently.
Track production per clinical hour (doctor and hygiene) and pair it with collection ratio. Some benchmarking sources cite hygiene production targets around $150 per hygiene hour as a reference point for many general practices. The exact number varies by geography and fee schedules, but the logic is stable: hourly production exposes whether time is being converted into the right mix of procedures with the right cadence.
The consequence of ignoring this metric is subtle. You can grow “busy” while profitability stays flat because time is being consumed by low-yield patterns, reappointments, and avoidable inefficiencies.
Accounts receivable is not a back-office report. It is cash flow risk. Once balances age, collection probability drops, and the effort required to recover them rises.
Track A/R aging mix daily (0–30, 31–60, 61–90,90+), and track days in A/R. Many revenue cycle discussions flag that A/R drifting beyond 30 to 40 days can indicate process breakdowns in claims, posting, and follow-up. Other dental benchmarking guidance emphasizes keeping the 90+ bucket small, often framed as best practice ceilings for long-aged balances.
The consequence is obvious on paper and painful in reality. You end up “profitable” on reports but cash-poor in operations, which then delays hiring, upgrades, and marketing decisions.
Patient retention failures rarely announce themselves. They show up as silent attrition: fewer reappointments, fewer family referrals, fewer follow-through visits.
Track reappointment rate, plus treatment follow-up latency: how many days it takes, on average, to move from diagnosis to first scheduled treatment appointment. Also track conversion for inbound leads, even if it is basic: inquiries to scheduled consult, consult to first visit.
The consequence is that growth becomes fragile. You spend to acquire demand that you could have retained with basic operational discipline and timely follow-up.
Forward-looking clinics are treating the dashboard as an operational intelligence layer in dental intelligence software, not a monthly reporting screen. In that context, systems like scanO Engage tend to be adopted because they combine an AI-powered dashboard for practice visibility with workflow execution: disease-wise insights, integrated AI soft tissue screening context, automated scheduling signals, digital prescriptions, smart patient calling, daily workflow management, and billing support. The goal is not “more data.” It is fewer blind spots, faster decisions, and a clinic that runs on leading indicators instead of end-of-month surprises.
The practices that improve fastest are usually not the ones with the most patients.
They are the ones that can see, daily, what is about to go wrong, and correct it while the cost of correction is still low.
An AI-powered co-author focused on generating data-backed insights and linguistic clarity.
Dr. Vidhi Bhanushali is the Co-Founder and Chief Dental Surgeon at scanO . A recipient of the Pierre Fauchard International Merit Award, she is a holistic dentist who believes that everyone should have access to oral healthcare, irrespective of class and geography. She strongly believes that tele-dentistry is the way to achieve that.Dr. Vidhi has also spoken at various dental colleges, addressing the dental fraternity about dental services and innovations. She is a keen researcher and has published various papers on recent advances in dentistry.








