
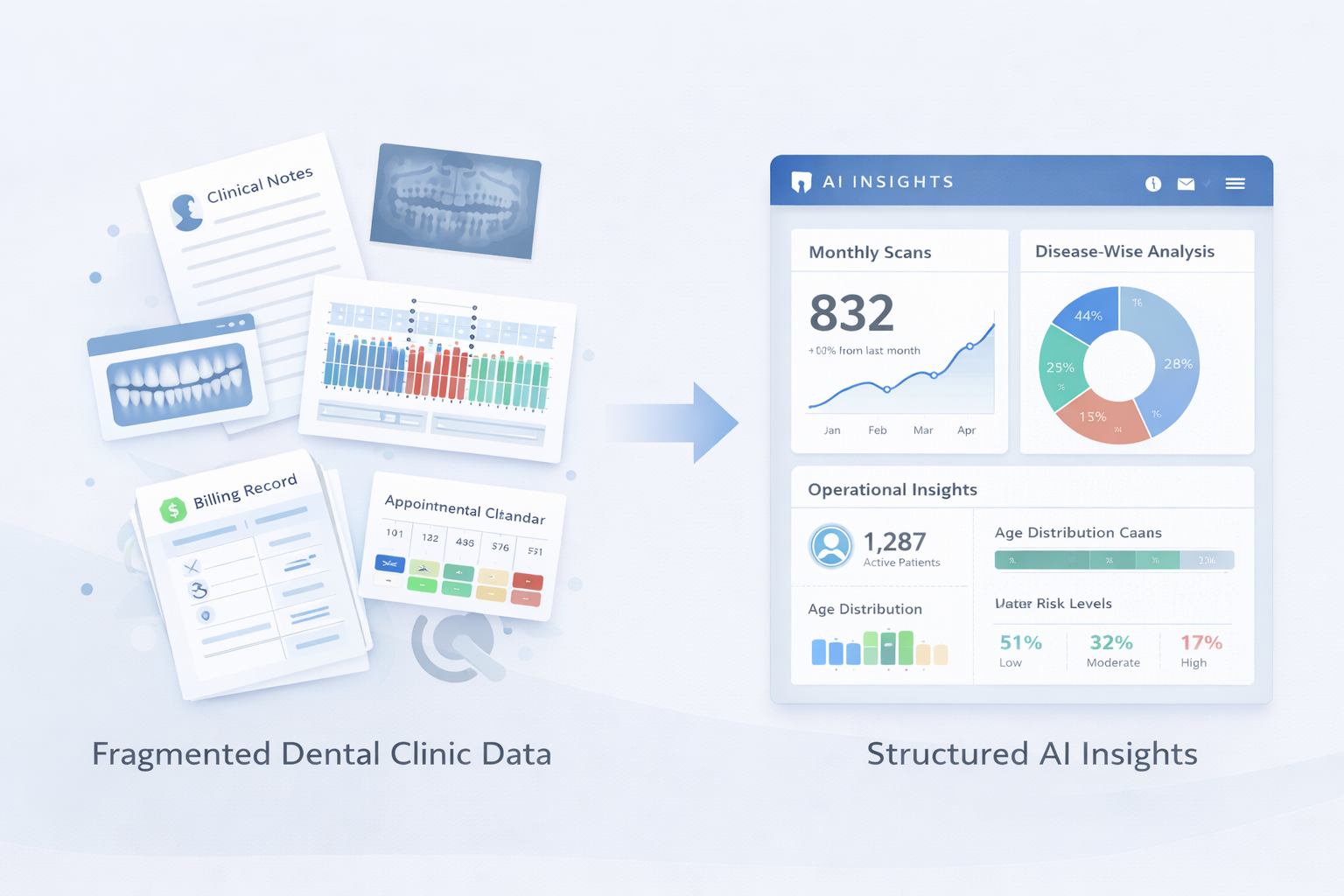
Most dental practices already generate plenty of data. Chairside notes, diagnosis codes, periodontal charts, radiographs, soft tissue observations, prescriptions, billing, cancellations, and follow-ups. The hidden problem is that this information is stored as disconnected fragments, so it cannot reliably answer operational questions like: Which conditions are rising, which patients are drifting, and where time and revenue are quietly leaking?
This is where AI for Automated Dental Analysis becomes practical. Not as a replacement for clinical judgment, but as a way to convert routine inputs into structured signals. When the same clinic data is consistently classified, trendable, and comparable, it becomes usable for decision-making, not just record-keeping.
The consequence of not solving the meaning problem is predictable. Clinics stay busy but remain uncertain about why performance shifts, why acceptance fluctuates, and why recall outcomes vary month to month.
Many clinic owners assume disease tracking is a “nice-to-have” that can be reviewed quarterly. The hidden issue is speed. Disease patterns move faster than quarterly reviews, especially when the clinic scales, adds associates, or runs outreach camps.
Globally, oral diseases affect close to half the world’s population over the life course, which means demand signals are always present, but they show up unevenly across age groups, neighborhoods, and patient cohorts. If your internal Dental Disease analytics cannot surface changes early, you discover them late, after schedules, treatment mix, and chair time are already impacted.
Dental AI helps here by automating classification and aggregation. Instead of asking staff to manually tag conditions, build spreadsheets, and reconcile mismatched notes, automated analysis turns recurring clinical observations into consistent categories. The value is not the dashboard. The value is that trends become visible while there is still time to adjust staffing, recall campaigns, preventive education, and chair allocation.
The consequence of slow analytics is that the clinic keeps reacting to symptoms, not managing patterns.
A common misconception in Dental data Analytics is that more fields, more forms, or more software entries create better visibility. In practice, more data often creates more noise because it is not comparable. One clinician writes “generalized gingivitis,” another writes “gum inflammation,” a third records bleeding points without interpretation. The data exists, but it cannot be rolled up.
This is a core issue in Data Analytics in Dentistry. Comparability is what allows you to answer questions like:
AI for automated analysis can standardize terminology and map variations in clinical language into consistent diagnostic buckets. It can also connect those buckets to outcomes like acceptance, recall adherence, and revenue mix, without requiring the team to become data specialists.
The consequence of non-comparable data is that management decisions get based on anecdotes: “It feels like perio cases increased,” or “It seems like patients are postponing.” That is not strategy. That is guesswork.
Many owners treat documentation and coordination as a fixed cost of running a clinic. The hidden problem is that it scales faster than revenue if you do not control it. Observational research in oral health teams has shown dentists spending meaningful portions of time on documentation, alongside consultation and other tasks. Even when the exact percentage varies by setting, the pattern is consistent: administrative load quietly consumes capacity.
This is one of the most under-discussed sources of growth limitation. If clinicians spend more time documenting, calling, re-calling, and coordinating, the clinic either reduces clinical throughput or increases staffing costs. Either way, margins compress.
AI-driven automation can reduce the manual burden by pulling insights from what is already being recorded and surfacing exceptions that need attention, instead of forcing teams to manually review everything. Evidence from broader clinical settings shows that automation can reduce documentation time after adoption, while visit volume can rise as workflows stabilize. Dentistry is not identical to primary care, but the operational logic holds: time recovered from repetitive tasks returns as usable capacity.
The consequence of ignoring operational friction is that “busy” becomes the clinic’s default state, and capacity becomes the ceiling.
Many clinics treat no-shows as random. The hidden problem is that no-shows are patterned, and when they are not tracked correctly, they distort operational planning. Research across healthcare contexts highlights that no-show rates can be substantial and economically damaging at scale. In dentistry, many practices report no-show ranges that can meaningfully disrupt chair utilization, especially for consult-heavy schedules and follow-ups.
AI-supported scheduling and follow-up systems can flag high-risk appointments, trigger reminders, and surface cohorts that repeatedly miss recall or treatment continuation. This matters because scheduling is not just a calendar function. It is a capacity allocation decision.
The consequence of unmanaged no-shows is not only wasted chair time. It is unreliable forecasting. Staffing decisions, lab coordination, and daily targets become harder to hit because the baseline assumptions are wrong.
The term Predictive Analytics in Dentistry is often misunderstood as something complex or academic. In a clinic, prediction is mainly prioritization: identifying who needs attention first, and why.
A practical predictive layer can answer questions like:
When AI for automated dental analysis connects diagnostic inputs to downstream behavior, it becomes possible to see where leakage occurs: at diagnosis, at explanation, at pricing, at scheduling, or at follow-up. That is when AI Insights Drive Dental Practice Growth, not by adding demand, but by reducing preventable loss in the demand you already have.
The consequence of operating without prioritization is that the clinic treats every follow-up as equal, spreads effort thinly, and misses the few interventions that would change outcomes.
The clinics that improve outcomes and efficiency are not the ones with the most software. They are the ones that turn daily activity into visibility: disease signals, conversion signals, scheduling signals, and workflow signals. Once visibility is reliable, decisions become calmer. You stop debating opinions and start managing patterns.
Forward-thinking practices increasingly close these gaps with AI-enabled practice intelligence platforms, for example scanO Engage, used as an operational intelligence layer rather than a reporting tool:
The reflective point is simple: clinics rarely underperform because they lack effort. They underperform because the signals inside their own data are trapped in fragments, arriving too late to shape decisions.
Frequently asked questions:
1. What does AI analyze during automated dental check-ups in a clinic?
AI uses clinic data like diagnostics, schedules, and billing records. It processes this information to create structured insights about disease patterns and how the clinic is performing.
2. How is analyzing dental disease data different from typical reports?
Instead of just showing past activities dental disease analytics looks at actionable trends and care gaps that need attention.
3. How does Tissue AI help improve clinical understanding and operations?
Tissue AI organizes data from soft tissue checks. It highlights patterns in oral lesion trends and gaps in follow-ups making them easier to see for both doctors and patients.
4. Can predictive analytics help dentists make better daily decisions?
Yes, it allows dental clinics to focus on the most pressing patients, conditions, or tasks making their work more efficient.
5. Does AI-based dental analytics take over a dentist’s judgment?
No, it provides steady and quick insights into trends that are hard to spot by hand supporting a dentist’s decisions instead of replacing them.
An AI-powered co-author focused on generating data-backed insights and linguistic clarity.
Dr. Vidhi Bhanushali is the Co-Founder and Chief Dental Surgeon at scanO . A recipient of the Pierre Fauchard International Merit Award, she is a holistic dentist who believes that everyone should have access to oral healthcare, irrespective of class and geography. She strongly believes that tele-dentistry is the way to achieve that.Dr. Vidhi has also spoken at various dental colleges, addressing the dental fraternity about dental services and innovations. She is a keen researcher and has published various papers on recent advances in dentistry.








