
Dental clinics have never lacked data. They lack usable truth.
Most practices can pull production reports, appointment lists, billing summaries, and basic patient counts. The misconception is that visibility naturally follows from having these exports. In reality, spreadsheets and static reports often increase confidence faster than they improve decisions.
That is the operational gap Dental Intelligence software is designed to close. Not by creating more reports, but by converting scattered operational signals into decision-grade insights: what is changing, why it is changing, and where margin or patient outcomes are quietly leaking.
Dental AI has quietly changed this dynamic by enabling clinics to interpret clinical and operational signals in real time, rather than relying on static reports.
A report tells you what happened. An insight helps you understand what is happening.
Most dental reporting is retrospective, aggregated, and slow. That makes it useful for accounting, but unreliable for daily management. The moment you run a clinic on last month’s totals, you start managing averages instead of behaviors.
This matters because dentistry is a throughput business with clinical complexity. Small variations in attendance, chair utilization, case acceptance, and claim outcomes compound quickly. The American Dental Association highlights benchmarks like keeping overhead near 63% or less of income and case acceptance in the 75% to 80% range as indicators of practice health. When those drift, the causes are rarely visible in a static month-end report.
Dental Intelligence software shifts the unit of management from “monthly totals” to “operational drivers,” so owners can see performance as a set of controllable levers rather than a surprise outcome.
Clinics often frame inefficiency as an isolated problem: no-shows, cancellations, delayed claims, incomplete notes, or slow follow-ups. The more accurate view is that these are symptoms of the same issue: variability that is not measured early enough to be corrected.
Take no-shows. Across healthcare, systematic reviews commonly find no-show rates around the low-to-mid 20% range, varying heavily by setting and population. In dentistry specifically, rates are often discussed in a broad band (commonly cited in the 10% to 30% range), which is operationally plausible because lead time, patient mix, and reminder systems vary dramatically by clinic.
The point is not the exact percentage. The point is that even small shifts are expensive because the unit cost is chair time.
A “15% no-show rate” is not only lost production. It is staff idle time, schedule instability, lower hygiene reappointment momentum, and compressed chair utilization that forces rushed clinical work later in the day. If you treat no-shows as a front-desk problem instead of a system behavior, you will keep paying for them.
A modern Smart Dental Clinic dashboard should not merely display attendance. It should surface patterns that predict attendance risk (lead time, time-of-day, patient history, procedure type), and show the downstream impact on chair utilization and production mix. That is the difference between monitoring and managing.
Owners typically track what is easy:
These are activity metrics. They are not useless. They are incomplete.
What drives practice economics is conversion quality:
The ADA’s case acceptance benchmark (75% to 80%) is a practical example. If your clinic is below that, the corrective action is rarely “sell better.” It is more often a breakdown in communication clarity, diagnosis consistency, financing friction, or follow-up discipline.
A good AI-powered dental dashboard for clinic performance tracking makes this measurable without requiring the owner to manually stitch together clinical notes, consult data, and billing outcomes. It connects the story across the patient journey: screening findings → treatment plan created → acceptance behavior → scheduling completion → claim outcome.
Without that connection, teams argue based on opinion:
With decision-grade visibility, you can isolate the true constraint: dental chair supply, case presentation workflow, follow-up latency, or payer friction.
Claim denials and delays are not rare edge cases. They are predictable failure modes of documentation, eligibility, coding, and workflow discipline.
A PubMed-indexed study of a large dental plan found an overall denial frequency of 8.2% of procedures, with the majority categorized as administrative. Even if your setting is different, the implication is consistent: a meaningful portion of revenue cycle friction is operational, not purely payer behavior.
When claim issues are reviewed manually once a month, they become “insurance headaches.” When they are measured daily, they become process defects:
Dental Intelligence software helps by turning denials into categorized signals, not anecdotes. It should answer:
That is how a clinic moves from coping to controlling.
Many clinic owners separate clinical quality from business operations, as if the data belongs in different universes. That separation is costly.
For example:
If you want to run a clinic like a stable business, you need a unified view of performance that respects clinical nuance. That is why an AI Dental Analytics software is not simply a business dashboard with prettier charts. It must integrate clinical signals in a way that supports decisions without turning the clinic into a data-entry factory.
Another misconception is that AI in operations is about replacing judgment. In practice, the operational win is consistency.
A clinic’s outcomes often vary by:
These variations create noise. Noise hides problems. And hidden problems become “normal.”
Dental practice analytics software for data-driven decision making can reduce noise by standardizing workflows:
In other words, AI is not the strategy. It is the enforcement layer for a strategy that already makes sense.

A practical definition is simple: it helps the owner answer the questions that normally require manual investigation.
Here are the questions that matter:
1) Where is time being lost today?
Not in theory, but in today’s schedule: gaps, overruns, and avoidable idle chair time.
2) What changed this week compared to last week, and why?
Not “production is down,” but whether it is driven by attendance, provider availability, procedure mix, or payer delays.
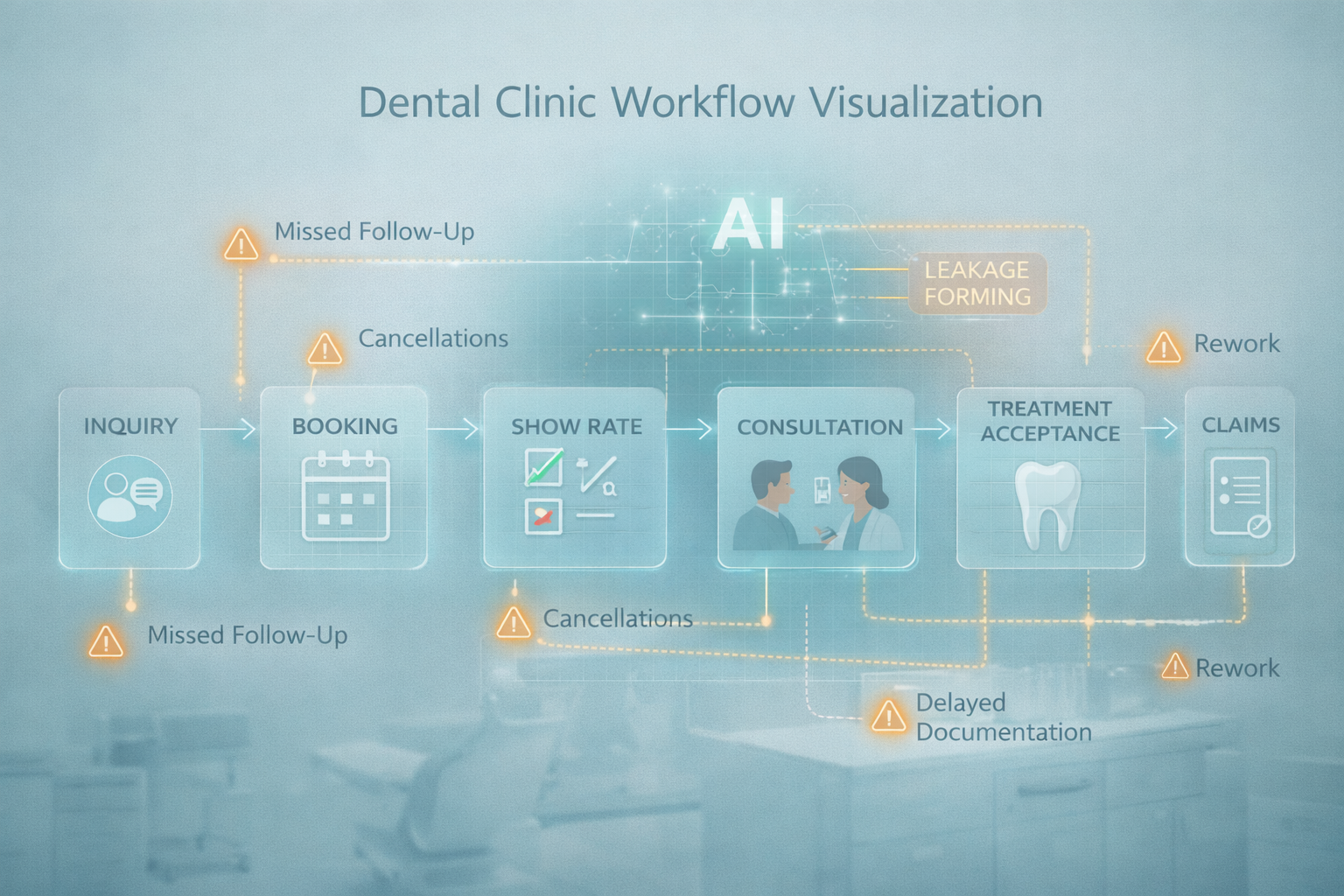
3) Which part of the patient journey is leaking?
Inquiries → bookings → shows → consult completion → treatment acceptance → scheduled completion.
4) Which behaviors predict future underperformance?
Rising lead time, increasing cancellations, slower follow-up, higher administrative denials, falling acceptance for specific categories.
5) What should be addressed first?
A prioritization layer matters because owners have limited attention. A dashboard that lists 40 metrics is not helpful if it cannot rank what is operationally urgent.
This is where the term AI Dental Dashboard earns its place. It is not a visual layer. It is a decision layer.
When dashboards fail, it is usually because they are built for observation rather than management.
Observation dashboards show:
Management dashboards show:
The difference is not cosmetic. It changes daily behavior.
A management-grade dashboard reduces the need for “end-of-month explanations” because it makes issues visible early. That is how clinics avoid the familiar pattern:
Over time, Dental Intelligence software becomes less about measurement and more about operational discipline. It creates a shared language that replaces guesswork with evidence.
Most practices do not underperform because the team is careless. They underperform because the clinic is managed through fragments: one tool for appointments, another for billing, another for clinical notes, and a spreadsheet to reconcile the gaps.
That fragmentation makes problems feel normal. And normal problems do not get solved. They get absorbed.
Forward-thinking clinics respond by building an operational intelligence layer that unifies performance signals into daily decisions. Systems like scanO Engage are examples of this approach when they combine an AI-powered dashboard for practice visibility with integrated workflows such as soft tissue screening inputs, disease-wise insights, automated scheduling, digital prescriptions, smart patient calling, daily workflow management, and billing support. The value is not the feature list. The value is closing the gaps between what is happening in the clinic and what leadership can actually see in time to act.
An AI-powered co-author focused on generating data-backed insights and linguistic clarity.
Dr. Vidhi Bhanushali is the Co-Founder and Chief Dental Surgeon at scanO . A recipient of the Pierre Fauchard International Merit Award, she is a holistic dentist who believes that everyone should have access to oral healthcare, irrespective of class and geography. She strongly believes that tele-dentistry is the way to achieve that.Dr. Vidhi has also spoken at various dental colleges, addressing the dental fraternity about dental services and innovations. She is a keen researcher and has published various papers on recent advances in dentistry.








