
Dental AI has quietly reshaped what a modern clinic looks like. Tissue AI can flag soft tissue abnormalities during a routine scan. Yet at the end of that same consultation, most dentists are still tearing a prescription off a paper pad and handing it across the counter.
That chit leaves your hand and immediately becomes invisible to you.
No record in the patient file. No dosage cross-check. No way of knowing, six months later, what was prescribed or whether the patient ever filled it. Multiply that across thirty patients a day and the documentation gap becomes significant. One insurance query, one complaint, one drug interaction, and the absence of a clean record stops being an inconvenience. It becomes a liability.
E-prescription for dental practice is not a new concept. What has changed is how seriously the regulatory and insurance environment is now treating documentation quality.
Insurance providers want structured prescribing records. ABDM frameworks in India are pushing healthcare toward digital health data. Patients who receive WhatsApp reports from their physician walk into a dental clinic and notice when nothing has changed. The contrast registers.
Paper prescriptions fail on documentation quality, clinical defensibility, and patient confidence. All three of those things have financial consequences.
No prescribing history at the next visit. A handwritten prescription from six months ago does not follow the patient. The dentist seeing them next starts from scratch. The treatment connection is broken before the consultation begins.
Dosage inconsistency across dentists. Two dentists in the same clinic often prescribe the same drug at different doses for comparable conditions. Neither knows. The inconsistency is invisible until a complaint makes it visible.
Pharmacy errors from illegible writing. A pharmacist who cannot read the prescription either guesses or calls the clinic. One creates a clinical risk. The other interrupts a busy session.
No delivery confirmation. The clinic has no way to know if the patient received, read, or acted on the prescription. If they lost it, they call back or skip the medication. Either outcome costs the clinic time.
No audit trail. When a regulator, insurer, or patient raises a prescribing question, paper files either exist or they do not. Incomplete, undated, or illegible records do not hold up in a formal review.
The shift from paper to an AI-enabled e-prescription tool for dental practice is not just a format change. The underlying architecture is different.
Paper is a one-way transaction. The dentist writes, the patient receives, and nothing is recorded. A connected electronic dental prescription management software creates a structured layer. The prescription links to the diagnosis, the treatment plan, and the patient's full clinical history in one view.
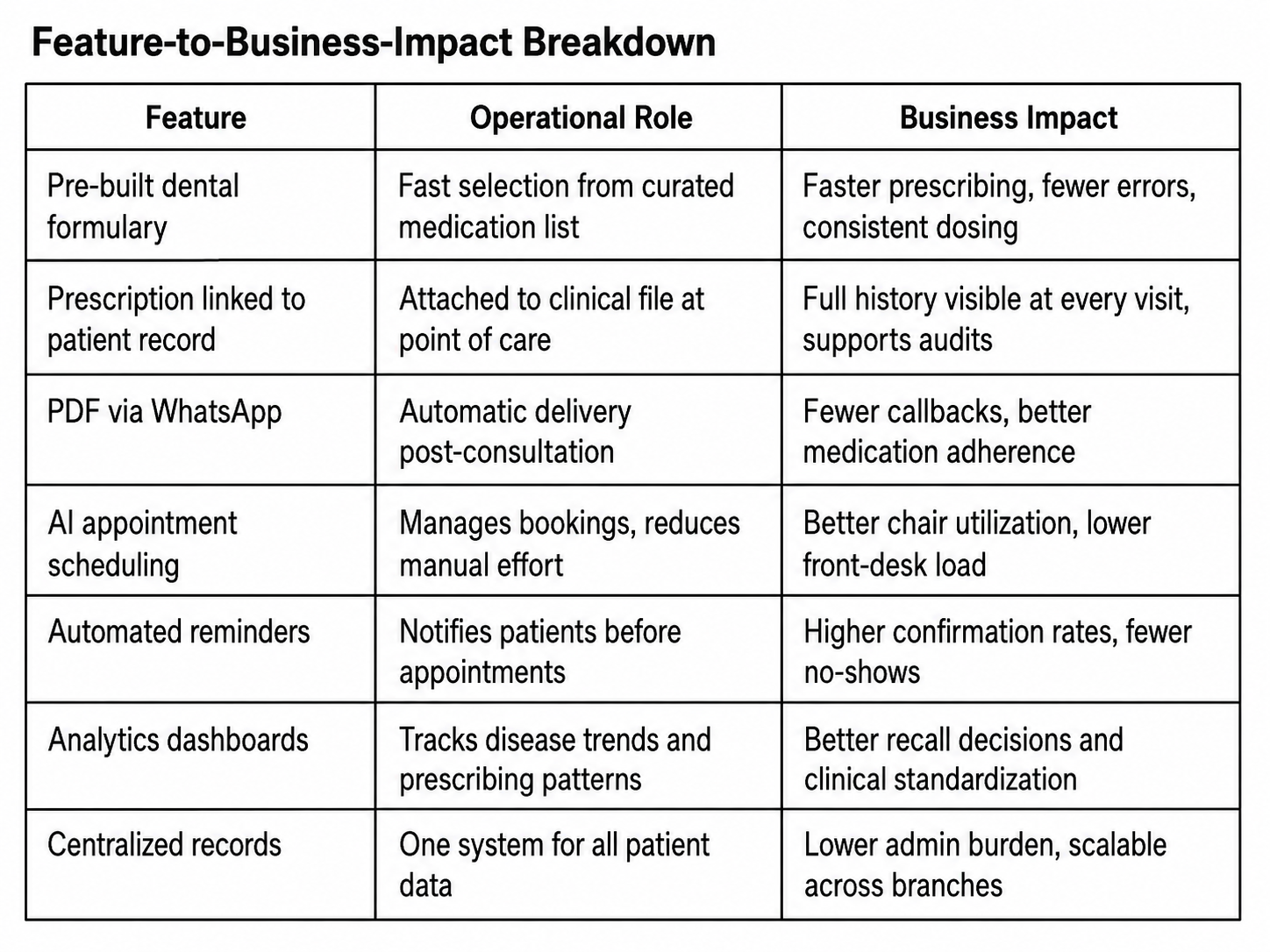
The most immediate difference is the formulary. A pre-built dental drug list means the dentist selects from commonly prescribed medications with standard dosage defaults already loaded. Antibiotics, analgesics, anti-inflammatories. The ones you write from memory every day. Selecting and confirming takes less time than writing by hand. The result is cleaner, faster, and immediately attached to the patient record.
Choosing the best e-prescription software for dentist use means looking for this connected architecture, not just a digital notepad.
Platforms like scanO Engage go further. The prescription is created alongside the treatment plan in one consultation session, linked to AI scan data from the scanO air robot. The completed prescription goes to the patient as a PDF on WhatsApp automatically. The clinic keeps a timestamped delivery log. Because appointment scheduling, reminders, and confirmation tracking all run in the same system, the prescription does not sit in isolation. It becomes part of a clinical record that builds over time and travels with the patient across visits and branches.
Best E Prescription software for dentist creates friction before it reduces it, if the rollout is handled badly.
Setup is front-loaded. The formulary needs to be configured before the system goes live. If it is not, the dentist searches through a generic database to find medications that should have been pre-loaded. That experience ends most transitions before they start.
The team needs to be trained together. A dentist who understands the workflow but whose assistant does not creates inconsistency. Everyone who touches the patient experience needs to understand what changed and why.
A standalone tool creates a new silo. An e-prescription tool for dental practice that does not connect to patient records, appointment history, or clinical scan data only solves the paper problem on the surface. The prescription exists digitally but is not visible where it matters, inside the patient's full clinical profile.
The cost feels unjustified on day one. For solo practitioners, a subscription for what appears to be a notepad replacement is a hard sell. That perception shifts around month three, once fewer callbacks, cleaner audits, and consistent prescribing patterns become visible in daily operations.
The clinics that abandon digital prescribing did not fail because the technology was wrong. They failed because the setup was incomplete.
A clinic that moves to AI-enabled dental e-prescription software does not just get cleaner records. It gets a foundation for better clinical decisions.
Prescription history informs the next consultation. Analytics surface untapped treatment opportunities. Disease-wise insights allow targeted recall campaigns based on actual patient data rather than guesswork. For multi-branch operators, centralized prescribing data is what makes clinical standardization possible across locations without depending on informal practitioner habits.
The transformation looks small from the outside. From inside the clinic, it changes how every consultation starts, how the team manages follow-ups, and how the owner understands what is actually happening across the practice.
We have been on paper for years without major problems. Why switch now?
The problems are mostly invisible until they are not. No audit was requested, until one is. No complaint needed documentation, until one does. Building the infrastructure proactively is significantly cheaper than retrofitting it under regulatory pressure.
How is this different from just typing a prescription into a notes app?
A notes app creates a text document. Good e-prescription dental software creates a structured clinical record linked to the patient profile, searchable by medication and date, delivered automatically, and visible at the next visit. An audit trail is built in. A notes app provides none of that.
What if patients still want a printed copy?
Most platforms support in-clinic printouts alongside WhatsApp PDF delivery. The digital record is created either way. Most patients shift to preferring the WhatsApp version once they realize they can access it from anywhere.
Is the AI component actually useful or just marketing language?
It matters most in the integration layer. When prescription data connects to scan findings, treatment history, and disease-wise analytics, the system surfaces patterns that paper records never could. The formulary delivers immediate value. The connected analytics deliver long-term value.
An AI-powered co-author focused on generating data-backed insights and linguistic clarity.
Dr. Vidhi Bhanushali is the Co-Founder and Chief Dental Surgeon at scanO . A recipient of the Pierre Fauchard International Merit Award, she is a holistic dentist who believes that everyone should have access to oral healthcare, irrespective of class and geography. She strongly believes that tele-dentistry is the way to achieve that.Dr. Vidhi has also spoken at various dental colleges, addressing the dental fraternity about dental services and innovations. She is a keen researcher and has published various papers on recent advances in dentistry.







